PELVI-URETRIC JUNCTION OBSTRUCTION (PUJO) (also- Ureteropelvic junction obstruction- UPJO)
Definition
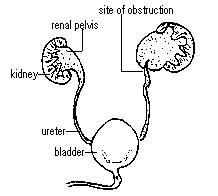
One of the main jobs of the kidney is to filter the blood, and then these waste products go via urine to the bladder. The urine leaves the kidney, enters the renal pelvis, and then passes into the ureter through a funnel called the pelvi-ureteric junction(PUJ). In some children, there can be a partial block at the PUJ. The block may be severe (high grade), minimal (low grade) or intermittent.
Symptoms of PUJ obstruction
The obstruction is usually due to an abnormality in the development of the muscle at the PUJ and causes urine to collect in the kidney. We detect many patients with PUJ problems before birth because of enlargement of the kidney (hydronephrosis) seen on the prenatal ultrasound. Older children may have pain (related to the blockage), urine infection (due to stagnation of urine caused by the PUJ blockage), or kidney stones. Prolonged blockage, particularly with infection, can damage the kidney. Sometimes, the block can be due to abnormal blood supply to the kidney.
Diagnosis
➾ Ultrasonography (USG) is the basic screening test which tells about the degree and severity of hydronephrosis (enlargement of the kidney) related to the PUJ obstruction.
➾ Nuclear Renal Scan or a Diuretic renal scan (DRS) is done to evaluate the urinary flow across PUJ and function of the kidneys. The best scan for this is a EC scan or a MAG3 scan.
Treatment of PUJ Obstruction
Antenatally detected PUJ Obstruction if not very severe is observed and a regular USG is done to see for any increase in severity. Also, a renal scan is done to make sure that the kidney function is preserved while waiting. Almost 60-70% of these children become better within the first 2 years of age and the hydronephrosis decreases. While in others, surgery may be required. Indications of surgery
➾ Increasing hydronephrosis
➾ Decreasing kidney function
➾ Decreasing kidney cortex on USG
➾ Symptoms in form of pain, infections, Hematuria
The usual repair of a PUJ obstruction (pyeloplasty) involves removing the blockage, and reconnecting the ureter to the renal pelvis. Depending on the individual circumstances, a tube may be left across the pyeloplasty (DJ stent) or a tube may be left above the repair to decompress the kidney (nephrostomy).
Technique of Surgery
The basic steps of pyeloplasty as mentioned above remain the same. The first step is to do a Cystoscopy and a Retrograde pyelogram (RGP). This a special x-ray study done under anesthesia to confirm everything before surgery and also to decide the exact site of incision.
➾ Conventional Open surgery: Pyeloplasty is performed by a small incision on the back and side of the tummy.
➾ Laparoscopic Pyeloplasty: The area of block is approached by key hole laparoscopic approach. Laparoscopic pyeloplasty is one of the most challenging reconstructive surgeries in pediatric laparoscopy. It involves dissection of the pelvi-ureteric junction, excision of junction & excess pelvis and then re-stitching the junction back properly through a telescope and two small key hole incisions on the belly. Laparoscopic pyeloplasty may take a slightly longer time than open surgery, but is compensated by a fast recovery and less pain post-operatively. There are hardly any stitch marks on the belly. Laparoscopic pyeloplasty is technically difficult in children less than one year of age due to the limitation of the working space in the belly and longer anesthesia times in smaller babies, but the post-op pain is much less and recovery is very fast, making it worthwhile to do a pyeloplasty laparoscopically.
Follow-up after pyeloplasty (repair of PUJ obstruction)
The DJ stent is removed after 6-8 weeks by cystoscopy under a short sedation at 6-8 weeks after surgery.
Ultrasound is done after about a month of stent removal and a renal scan 3-4 months later. A child should be followed up for at least several years after a pyeloplasty. Even after successful repair of a PUJ obstruction, the hydronephrosis in the kidney may persist and an ultrasound may still “look abnormal”. Tests that evaluate kidney function, such as the renal scans, are better ways to follow children after repair.
